The soft toric lens market represents a disproportionate number of patients in this modality. One only has to look at the demographics of the number of astigmats in the population to realise there is a serious underuse of toric contact lenses. It has been estimated that 39% of the population have at least 0.75D of astigmatism, but when we analyse the work of Morgan et al (1) the overall global use of soft torics was 23% in the year 2005. Morgan quotes a range of 3% soft toric use in Greece, to 40% in Sweden. So why this dichotomy, why do some countries have such a high use whilst other do not? There are a number of potential answers to this question, but without doubt patient satisfaction is not as high with soft torics as spherical soft lenses. Young et al (2) re-fitted 236 lapsed contact lens wearers. Short term success was measured at one month and telephone interview at 6 months. The soft toric wearers did poorly against their spherical counter parts with only 69% being successful as opposed to 91% with 2-week reusable spherical lenses. At 6 months this figure had declined further to 42%. In another study conducted by Hickson-Curran et al (3) only 70% of the 335 astigmats surveyed described their overall opinion of their conventional soft toric lenses as “excellent” or “very good”. More importantly only 65% rated their comfort with these lenses as “excellent” or “very good”. When the study group was asked if their soft toric lenses met expectations 25% said they were “much worse” or “slightly worse”. So clearly conventional soft toric lenses are not as successful as spherical lenses. The reason for this is multifactoral, but at the top of the list is comfort and vision. If clinical success is to be achieved with soft torics, these two factors have to be addressed.
The challenge
It is an inherent disadvantage that soft toric lenses move on the eye, and just a 5° off-axis movement can be enough for the perceptive patient to notice. Over the past few years great strides have been made to not only improve stabilization, but also the speed of stabilization.
Without doubt the main reason for the discontinuation from conventional soft toric lenses is discomfort. The reasons these lenses are less comfortable than their soft spherical counterparts is also multifactoral. Poor wetting and incomplete blinking plays a major role in the thinning of the pre-corneal tear film. It must be remembered that soft lenses do not rotate like conventional spherical lenses, and quite frequently a tide-mark can be observed just beyond the leading edge of the upper lid. Much of the drying effects of soft torics account for the short term feeling of discomfort, but what role does hypoxia play in the cases of chronic discomfort?
Dk and Soft torics
As Eye Care Practitioners (ECP’s) it is our moral, ethical, and professional role to provide our patients with contact lenses that do not compromise their Ocular health in any way. Avoiding hypoxic changes of the cornea should be uppermost in the thinking of the vigilant ECP. Over the last twenty years a great deal of research has been conducted into how much oxygen the cornea requires, in both the closed and open eye. Harvitt & Bonanno (4) concluded that a Dk/t of 35 was required to avoid stromal anoxia in open eye conditions (our daily wear patients). This exceeded the Holden & Mertz criteria of 24 Dk/t and has now become the target for lens designers. With this in mind how do present hydrogel soft torics compare against the target of 35 Dk/t? In 1996 Eghbali et al (5) analysed a range of medium water content {45 – 70%} prism ballasted soft torics.  They measured thickness at various points across the lens and then calculated the Dk/t. At 6 mm beneath the centre of the lens they found an average thickness of 0.40 mm ± 1.56, giving an average Dk/t of 3.40 ± 0.3. Clinically this is unacceptable as it could well be the catalyst for hypoxic changes of the cornea such as neovascularization {Fig 1}, limbal hyperaemia, and epithelial microcysts. There is a great deal of anecdotal evidence that these changes contribute to reduced “end of day” comfort and the patient’s eventual discontinuation from soft torics. The Oxygen maps in fig 2 illustrate quite clearly the stark contrast between the oxygen transmissibility’s of the conventional soft toric and the Silicone-hydrogel toric. The ECP should also bear in mind the prescription. As more and more Hyperopes are considering part time wear oxygen transmissibility becomes more of an issue. They measured thickness at various points across the lens and then calculated the Dk/t. At 6 mm beneath the centre of the lens they found an average thickness of 0.40 mm ± 1.56, giving an average Dk/t of 3.40 ± 0.3. Clinically this is unacceptable as it could well be the catalyst for hypoxic changes of the cornea such as neovascularization {Fig 1}, limbal hyperaemia, and epithelial microcysts. There is a great deal of anecdotal evidence that these changes contribute to reduced “end of day” comfort and the patient’s eventual discontinuation from soft torics. The Oxygen maps in fig 2 illustrate quite clearly the stark contrast between the oxygen transmissibility’s of the conventional soft toric and the Silicone-hydrogel toric. The ECP should also bear in mind the prescription. As more and more Hyperopes are considering part time wear oxygen transmissibility becomes more of an issue.
At the present time there are three Silicone-hydrogel torics available to the practitioner.Table 1 below illustrates the three lenses that are now available. All three have good oxygen permeability, and made in the majority of powers will meet the Harvitt& Bonanno criteria of Dk/t 35 for daily wear. Consideration should be given to lens modulus as this can have an impact on the way the lenses fit especially if the patient has a history of CLPC.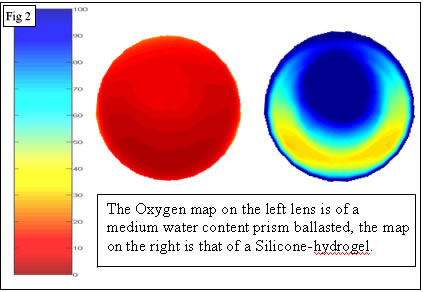
Both Manufacturers and ECPs, want the Industry to grow and the increased use of Silicone-hydrogels is one way to add to that growth. Rather than wait for your patient to come back to you with hypoxia related problems and reduced wearing times, be “pro-active” and refit them in Silicone-hydrogels before complications occur.
Table 1
| Silicone-hydrogel toric lens characteristics |
Lens |
Dk |
Dk/t @ -3.00 |
Water content |
Modulus |
Acuvue Advance for Astigmatism |
60 |
86 |
47 |
0.43 |
Air Optix Toric |
110 |
108 |
33 |
1.00 |
Purevision Toric |
99 |
91 |
36 |
1.50 |
References
- Morgan P et al International Contact Lens Prescibing in 2005 CL Spectrum 2006: Jan
- Young G et al A multi-centre study of lapsed contact lens wearers Ophthal. Physiol. Opt 2002 22: 516-527
- Hickson-Curran S et al Toric contact lens wearers: Where are we now? Optical Management Feb 2005
- Harvitt DM et al Re-evaluation of the oxygen diffusion model for predicting minimum c/lens Dk/t values to avoid corneal anoxia Optom Vis Sci 1999; 76: 712-719
- Eghbali F et al Oxygen transmissibility at various locations in hydrogel totic prism ballasted c/lenses Optom Vis Sci 1996 73;3: 164-168
|



